
By Nelly Kalu
Nigerian women shoulder the cost of surgery and contraception as the government prioritizes other health programmes.
Women of African descent are four times more likely to have uterine fibroids. Although many of these cases are asymptomatic and undiagnosed, published estimates say black women face a higher lifetime risk of up to 80% by age 50 globally. These high-risk factors are linked to genetics, hormones, and delay in care during the first five years of diagnosis. Yet in Nigeria, the most populous black nation on earth with nearly half the population women, are unable to access healthcare needed for this condition.
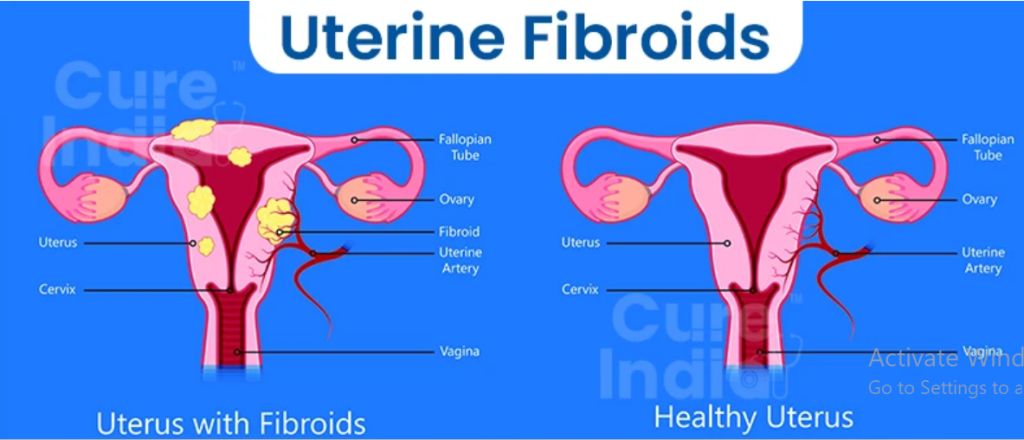
Uterine fibroids are benign tumours that affect the female reproductive system and “curable” by myomectomy, the surgical removal of the tumour from the uterine wall to preserve fertility. An expensive and emotionally draining decision for many women to make, especially because it is not a guaranteed solution for the problem. The only absolute cure for fibroids is hysterectomy, the surgical removal of the womb.
Depending on their size, number and location, the symptoms of fibroid are complicated and dangerous. It often presents— and this is not an exhaustive list— as heavy/painful periods, heavy bleeding between periods which often causes patients to become anaemic, pelvic pressure and constant urination, constipation and abdominal largeness, pain during sex, infertility. Although fibroid surgeries have become relatively safer today, with a low 0.2% mortality rate, with improved medical knowledge and non-invasive options such as uterine fibroid embolisation (UFE).
There are no assurances that fibroids once surgically removed do not return. Many women have undergone multiple surgeries for recurrent fibroids. Doctor Emeka Igbodike, co-author of the surgical report on fibroids, “Giant “Hydra Headed” Fibroid in a Nullipara” and an obstetrician-gyneacologist (OB-GYN) who has performed multiple fibroid surgeries in Nigeria and in United States, says that there is possibility of recurrence of fibroids tumours in about three to 27% of cases depending on a few factors such as the woman’s age and whether the fibroid nodules found are more than three.
“In fact, for every one Caucasian worldwide, up to four to nine African women have uterine fibroids. That’s how common it is with us [Africans].”
Public healthcare in Africa is challenging. In fact, this is where international donors and grants are most prominent and efficient. The public health sector was the most hit with the withdrawal of USAID and the reduction of global aid funds, but before the global aid cuts, there was always disproportionate care for female reproductive health. Most never suffer fibroid symptoms, and only discover it during routine pelvic exams.
High costs, weak policy, and fear keep fibroid care out of reach
In Nigeria, for instance where uterine fibroids affect nearly 80% of women of reproductive age. It was a surgery with recurrent casualty rates, mostly due to medical negligence, and even now, with more news of deaths in 2025, women still consider it a death sentence. In most cases, their complaints are dismissed by medical professionals leading to years of inattentive care and misdiagnosis. Today, although safer, uterine fibroid surgeries are very expensive. There is also a lack of data and supporting information for women to make informed choices about their treatment. Women in Nigeria are the poorest demographic, earning less than a dollar on an average yet there is no national health policy guiding or subsidising the cost of uterine fibroid care.
Amanda Chinedu still remembers her friend and roommate, Jessica*. They both served as missionaries under the Youth With A Mission (YWAM) in Port Harcourt, Nigeria. Jessica suffered increasingly painful periods and heavy bleeding that would cause days of pain and agony, unable to work or even experience a healthy quality of life in a country where the quality of life is precariously low. Unable to access safe and affordable healthcare when she needed it, she was eventually operated upon, during the COVID-19 pandemic, without any anesthesia and died.
Amanda recognised this pain because her sister suffered the same thing. Both women were afraid of the expensive fibroid surgeries. Many women are faced with a difficult decision; have the surgery or live with the pain. Contraceptive options that could mitigate the pain, providing some time to mentally and emotionally prepare for surgeries, are either very expensive or not presented as viable and accessible options by doctors.
Hormonal birth control pills prescribed without any education for the patient are counter-productive. Some doctors say they tend to make the fibroids “grow bigger”, but low dose or estrogen-absent pills do not have this effect and can relieve the bleeding. IUDs such as Mirena delay the growth process a little by injecting progesterone which in turn slows the growth of the fibroids. These measures are often better the earlier the woman is placed on them. But a single Mirena costs as high as ₦300,000(naira), while surgery ranges from ₦500,000 to ₦3,000,000 ($2000) without including the cost of tests or post-surgery care.
The fear associated with cost and presumption of death due to complications from fibroids surgeries is another reason women delay accepting a surgical resolution. Dr Igbodike calls it the “not-my-portion syndrome”. A term in Nigeria used to reject the possibility of a terrible situation or outcome and ward off any impending evil.

“So there’s emotional breakdown when you tell a woman for the first time, that uterine fibroid was found, sometimes incidentally in an ultrasound scan as some of the uterine fibroid can actually be asymptomatic. She starts to worry “I have fibroids, am I going to have babies again? [They] don’t want to be associated with fibroids even though we know that up to 99% of cases are benign.
Dr Igbodike also worries about the influence of religion on women who should seek a more permanent solution to the bleeding and pain caused by fibroids.
” You know, usually there’s this thing they call not my portion syndrome. Once you mention it, the woman will immediately reject being operated upon. So mentioning uterine fibroid is multifaceted in terms of the emotional sequence of what this woman is going to feel.”
There is a constant demand for fibroid care in Nigeria but no commitment to this problem in the country’s national healthcare agenda.
Rwanda treats fibroid care as a public good, while Nigeria leaves women to pay the price.
In Rwanda, IUDs like Mirena which supply progesterone in doses that help to balance the fibroid feeding estrogen are free for all women. Citizens and non-citizens alike.
This is possible in Rwanda because in 2020 the county introduced a national health insurance scheme that allows public hospitals to grant “no-cost contraceptives for all”. This scheme is known as Mutuelles de Santé and it centers on the Community-Based Health Insurance (CBHI). It provides cover for 92% of the population through equity, solidarity, and risk-sharing.
Speaking at a national press conference to reporters in Kigali, Rwanda, President Kagame addressed this approach to healthcare equity stating that it comes from valuing all members of society as equal and not approaching healthcare solutions in isolation. He recommends learning from others about the best way to provide equitable care for all members of society, especially women who make up half of every society.
“The first thing for people to have in their minds is the importance of women as a big part of the society. If you think of women and their specific needs, and build their involvement around that, you get the rest right. Therefore, in thinking about good health for your population, you must consider certain things that affect different groups. What are the specific needs? You break them down and create resources for each aspect. This is where it starts from. If you don’t start from here, the rest goes wrong.”
On the contrary, Nigeria has no national policy or program for fibroids, and the condition is absent from major health strategies. Advocates want fibroid care included under the NHIA to cover costly treatments like myomectomy and hysterectomy. Current responses are limited and uneven and not nationwide, such as occasional free surgeries at a few public hospitals like University of Port-harcourt Teaching hospital (UPTH), while NHIA support largely targets broader maternal health through the Vulnerable Group Fund.
Health financing is governed by the NHIA Act of 2022, which mandates insurance coverage for all residents. It links state insurance schemes and the Basic Healthcare Provision Fund, which has disbursed over ₦260 billion for primary care, prioritizing vulnerable groups like children under five and pregnant women. This insurance does not cover IUD’s, injectables or even fibroid surgeries. Where approximately 20-50% of Nigerian women of reproductive age (typically 15-49 years) have uterine fibroids.
Nigeria lags on contraceptive access and equity.
Dr. Ejike Orji is Nigeria’s representative to Family Planning 2030 (FP2030), a global coalition of about 85 countries working to expand access to rights-based family planning by 2030. He says Nigeria is underperforming on the modern contraceptive prevalence rate (mCPR). As of 2022–2023, only 15% of women aged 15–49 use a modern contraceptive method, far below FP2030’s target of 27% by 2030.
On the disparity between the cost of Mirena, Dr Orji clarifies; “Let’s take the three tier care system of Nigeria. If you go to a hospital, a private hospital, you have to buy Mirena at the highest price. If you go to a secondary facility, the price will come down a little bit. If you go to a primary health care center or a primary or a secondary facility in rural Abuja or semi-urban Abuja [the nation’s capital], there is a chance that you might get it for free. Most women don’t have this information. The price can range from 40,000 naira to 60,000 naira or for free in a place like Abuja”
This is termed the ‘total market approach’. Dr Orji is a strong supporter of this method for achieving female reproductive care equity. He describes the total market approach as one where the provision of, accessibility, and affordability of medical care is pegged according to socioeconomic class. Public hospitals subsidise, private hospitals charge at premium.
“That’s the only way we can make sure that services will be available to the average Nigerian, says Dr Orji. “Corruption is the biggest devil that we have in the country. So I’m completely in line and in tune with the total market approach. If it does properly, we can mobilize resources, and then that will be able to sustain services to the people who need them.”
Another measure the Nigerian government is implementing is the sector-wide approach or SWAp. Initiated by the Minister of Health and Social Welfare, Professor Muhammad Ali Pate, SWAp is a development method where the federal government and donors collaborate under a unified framework.
Local funding, policy pressure, and data tools offer a path forward for fibroid care.
With the withdrawal of USAID by the Trump government, many of these family planning programmes in Nigeria were rolled back affecting millions of women and girls dependent on it. This has reignited conversations around self funding health initiatives. To that end the government established the Medical Relief Fund, which has put about $200 to $300 million to the sector wide votes, which they intend to use to fill the gap of the American withdrawal for the country’s healthcare system.
In addition to this a female-led organisation called Youterus, based in Sierra Leone and dedicated to caring for, and gathering data on African women uterine health. The organisation’s first Africa-wide campaign on fibroid and endometriosis “Unmute the Womb” is making uterine fibroid care a priority. They have also created a fundraising mechanism, Uterine Health Fund, that supports the cost of surgeries for women in Nigeria and Sierra Leone, and an AI-powered tool, The Womb Index, that “identifies red flags, predicts risks, and guides earlier triage-strengthening clinical decision-making across thousands of women’s experiences.” “If uterine health is not visible in policy, it will not be measurable in data. And if it’s not measurable in data, it will not be financed.” says Fatou Wurie, CEO, Youterus on a LinkedIn post.

So far, the federal government increased family planning budgets through the sector-wide approach. Dedicating $6.1 billion to the National Primary Health Care Development Agency (NPHCDA) to strengthen primary healthcare, and establishing the Presidential Initiative for Unlocking the Healthcare Value Chain (PVAC). However, experts like Dr Orji are concerned about the lack of transparency in how these funds are procured and disbursed.
The tier-based provision of care and total market approach is how Nigeria intends to achieve health care equity. Unlike Rwanda, where healthcare initiatives are measured through a multi-gendered equity lens, for Nigeria, it is more of a socioeconomic approach. One that aims to provide care for those less privileged through subsidies. There are two main problems with this measure: if those in the lower socioeconomic classes have no information about this subsidised care, does it still serve them? And, when society is class-abstract of gender, women are often forgotten, becoming once again the opportunity cost in Nigeria’s healthcare gamble.